Testimony of Linda Andre, Director of Committee for Truth in Psychiatry
New York State Assembly, May 18, 2001
 My name is Linda Andre, and I am a survivor of ECT. I had a fairly typical experience. Five years of my life were permanently erased as if they had never happened, including most of my college education; I lost 40 points off my IQ; and I've been left with permanent disabling memory and cognitive deficits. I have brain damage from ECT, and it's very similar to what happens to persons who suffer traumatic brain injuries from other causes such as car crashes. Let me hasten to say that I received what's often falsely called the "new and improved" ECT and that every doctor who consulted on my case agreed and will tell you to this day that my treatment was state of the art and done according to the specifications of the APA. Since 1985, I have been the New York Representative of the national organization of persons who've received ECT, the Committee for Truth in Psychiatry; in 1992, I became the Director of our organization.
My name is Linda Andre, and I am a survivor of ECT. I had a fairly typical experience. Five years of my life were permanently erased as if they had never happened, including most of my college education; I lost 40 points off my IQ; and I've been left with permanent disabling memory and cognitive deficits. I have brain damage from ECT, and it's very similar to what happens to persons who suffer traumatic brain injuries from other causes such as car crashes. Let me hasten to say that I received what's often falsely called the "new and improved" ECT and that every doctor who consulted on my case agreed and will tell you to this day that my treatment was state of the art and done according to the specifications of the APA. Since 1985, I have been the New York Representative of the national organization of persons who've received ECT, the Committee for Truth in Psychiatry; in 1992, I became the Director of our organization.
I'd like to add that although I'm not a doctor, I passed the CME test that supposedly qualifies doctors to give shock. I've got the certificate to prove it.
The reason why there was and is a need for a national organization of ECT survivors is that there are big problems with this treatment, as you're hearing today. In a nutshell, the problem is that patients aren't truthfully informed of the known permanent adverse consequences of ECT, including permanent extensive memory loss and permanent brain damage. The industry, much like the tobacco industry, won't acknowledge these effects and ex-mental patients haven't got the political clout to make them.
Throughout the history of ECT, there has been conflict between doctors and patients. This conflict is at the very heart of the Paul Henri Thomas case, and the other forced shock cases in New York. What survivors know to be true about ECT, and what doctors believe, are opposed and are irreconcilable. Survivors and shock doctors cannot both be right. I sat through the Thomas court hearings, and I heard the doctors say that they considered Paul incompetent because he did not agree with their assessment of the risks and benefits of shock. I heard what the doctors said, and I don't agree with them either, nor would any of the members or our organization. I guess that makes all of us incompetent as well. Paul came to his conclusions by experiencing ECT. His doctors said they formed their opinions on ECT by reading a book. (There isn't major book on ECT that isn't written by a doctor with financial ties to the shock machine industry, as an owner, shareholder, grantee or consultant to these companies.) Paul's doctors believed things that are not true, such as that the FDA has performed safety trials of ECT; but then what matters in these hearings is not so much what is true as who has the power to define the truth.
Our group organized because we all had ECT without informed consent, we all suffered permanent memory loss, and we want to protect future patients from suffering tragically preventable amnesia and disability. Our one and only mission is to advocate for truthful informed consent, and we've done that over the past sixteen years in a wide variety of forums. In fact, Marilyn Rice, the founder of our group, testified before the New York Assembly at your first hearings on ECT in 1977. We called ourselves the Committee for Truth in Psychiatry to emphasize that we are for informed consent, not against ECT. Marilyn liked to say, "I'm not against ECT, I'm against lying about ECT."
In my position as Director of CTIP I've been in contact with literally thousands of ECT survivors from around the world over the past decade. I keep up with the industry research on ECT; I attend and present at psychiatric conferences; I write and publish on ECT; I consult with agencies such as the Center for Mental Health Services. I've worked with states which have passed or tried to pass laws to protect patients. This last includes an unsuccessful reporting bill in New York State in the early 90s, and reporting bills that were successful in Texas and Vermont. But CTIP's biggest accomplishment has been getting the Food and Drug Administration to acknowledge the risks of ECT, including brain damage and memory loss.
The FDA regulates ECT because the machines used to give it are considered medical devices. It is somewhat limited in its authority because ECT machines were in use before the FDA gained jurisdiction over medical devices in 1976. FDA was mandated by law to place the shock machines in one of its three medical devices categories, Class I, Class II, or Class III. Briefly, Class I would be an over-the-counter device, Class II one which is safe if used according to certain standards or safeguards, and Class III one which presents an unreasonable risk of injury or harm and cannot be made safe. To classify a device, FDA weighs its risks against its benefits. At the end of my presentation, I will tell you what the FDA says about shock machines. But first I will do what the FDA did, and give you an overview of what we know about ECT's risks and benefits.
ECT patients have been reporting permanent adverse memory and nonmemory cognitive effects ever since shock began in 1938. The nature and frequency of these reports has not changed in over 60 years. Let me explain that the so-called modifications of ECT have had no effect on these permanent adverse effects. You may have heard claims that oxygenation, muscle paralyzers, so-called brief pulse ECT, or unilateral ECT have solved the problems with memory loss and brain damage. But all of these modifications were in use by the 1950s, and none of them eliminated or minimized ECT's effects on memory and on the brain. You may also have heard that today's ECT uses "less electricity" than in the 50s, 60s, 70's, and 80s. The opposite is true. Today's ECT devices are the most powerful in history. Each new generation of machine is designed to put out more electricity than the one before it. This means, for example, that a person getting shocked today is probably getting more electricity through her brain than I did in 1984.
In the early decades of ECT, doctors were frank about sacrificing the brains, intellects, and careers of their patients in the hope of a temporary respite from depression. Since about 1975, the beginning of what I call the public relations era of ECT----that is, the period when organized psychiatry decided to deny there was any problem with ECT itself in favor of claiming there was simply an image problem with ECT---they have attempted to deny or cover up memory loss and brain damage, just as they have stopped writing up ECT deaths.
Even so, it is accurate to say that when researchers looked for the type of memory and cognitive deficits survivors report, and used measures that were relevant to these deficits, they have found them. There are just a handful of studies that follow ECT patients up for the long term, asking about memory. But the studies that have done this--followed patients for six months, a year, three years, and in one very brief and limited study, seven years---have all found that the majority of these patients still have amnesia and memory disability. There is nothing to support the industry's claim that memory or memory ability returns to normal shortly after ECT. In fact, patients tested as long as twenty years after ECT had brain damage verified by sensitive neuropsychological tests.
Outside of these of studies, which were done before 1990, no one has been interested in following up ECT survivors to document the permanent effects of ECT---except ECT survivors. Let me explain that survivors and others have had to step in because of the lack of ethical and scientific research, and this is something you may want to look into in further hearings because New York State is where the biggest problem is. You may know that one institution, the Psychiatric Institute, gets a large percentage of the total NIMH money that is available for mental health research. When it comes to ECT research money, the percentage is much greater. Millions and millions of dollars have been granted to one investigator in this lab, Dr. Harold Sackeim, to study ECT, including the adverse effects of ECT. Because Sackeim's had a lock on this money for 20 years, because his money is renewed automatically for as long as he wants it without his proposals having to compete with other grants, and because he sits on the panel which decides who gets funded, other researchers aren't able to get grants to do research in this area. Dr. Sackeim is on the American Psychiatric Association's Task Force on ECT, and he's the spokesman for industry, the one whose name is always given out to the media. His entire career has been built on promoting ECT. That's an ethical and scientific problem. But there's an even bigger legal problem: his research has been done in violation of federal law which requires disclosure of conflict of interest. While he's been getting millions of NIMH dollars, he's also been a consultant for, and received grant money from, the companies that make most of the shock machines in America, and he has never disclosed this financial conflict. That is illegal.
I also need to add that Dr. Sackeim, along with other New York ECT promoters such as Dr. Fink, and the other doctors of the APA's Task Force on ECT, are on record at the Food and Drug Administration as opposing an impartial safety study of the effects of ECT on the brain. They have successfully lobbied over a period of nearly two decades to prevent such a study by the FDA. So it is not only that these men monopolize the research funding and decide the research agenda; they also work to actively prevent anyone but themselves from researching ECT.
I hope you will look into this, and into other problems in this research as well, such as fraudulent informed consent, the "disappearing" of study participants with adverse outcomes, the fudging or falsification of data. All of this is documented. I bring it to your attention because there is no way to understand the dearth of valid and scientific research on longterm effects of ECT without placing it in this larger context.
So if the research money is monopolized by Sackeim and a handful of others with a personal financial and career stake in promoting ECT, how do we know what we know about the nature and prevalence of its adverse effects?
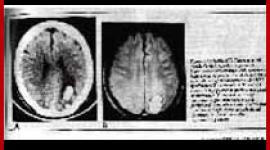
We know because of the research that was done prior to the public relations era, and in fact even up until the early 80s. There are dozens of brain anatomic studies of both humans and animals, autopsy studies where cells have been counted, solid scientific studies which have been replicated by other studies, showing brain damage from ECT. The industry tries, dishonestly, to discredit this research but there are too many studies. In fact, though they're either ignored or miscited by ECT proponents, there human MRI studies showing brain atrophy from ECT. There are also well-designed memory studies which have never been either discredited or replicated by the ECT industry, documenting the nature, extent, and permanence of ECT amnesia.
I refer you to the excellent presentation given by neuroanatomist Dr. Peter Sterling in 1977, in which he describes the mechanism by which ECT inevitably produces brain damage. The brain hasn't changed since 1977, and ECT hasn't changed except for the fact that today's ECT machines put out many times more electricity than those in use is 1977.
The permanent effects of ECT on the brains, memories, and lives of survivors are documented in the files of the FDA. The FDA has been collecting data from ECT survivors for nearly 20 years. Its docket on ECT, Docket #82P-0316, consists of about 40 volumes, each several inches thick, and I have read all of them. This is a public record and anyone making policy on ECT should look at it. There are several hundred reports from persons who have had ECT. They come from persons who had ECT at different institutions, at different times and in different places, but the similarity of the reports from these hundreds of survivors who don't know each other is unmistakable. They describe permanent amnesia and memory disability---the daily experience of living with a poorly functioning memory. Some have sent in laboratory tests documenting brain damage. They talk of losing jobs, forgetting the existence of children, becoming a permanently diminished human being. There are hundreds of reports of educations and careers ended, families destroyed. Many reports go into great detail about the nature of ECT disability, such as the fact that new learning after ECT doesn't stick. These people want something done about what happened to them. They beg the FDA to conduct an impartial safety investigation of ECT's effects on the brain.
There are exactly fourteen letters from patients who have anything good to say about ECT. Five were sent in by these patients' shock doctors, some of these written on hospital stationery, probably with the shock doctor literally looking over the patient's shoulder, telling them what to say. Four of the letters report memory loss.
That's fourteen letters in nineteen years from ECT patients who had positive experiences, versus several hundred who report negative, harmful, or devastating results.
This is and was not meant to be a scientific study but it is what we have to go on, and it has some advantages over a conventional study which would, after all, include patients all treated by the same doctor in the same institution, and would only include one or two dozen people. The ECT reporters had ECT in every decade, by every imaginable technique and type of machine, by every type of doctor, in every state and even some foreign countries. It's not possible to dismiss them by claiming they "just" had a bad doctor, or the wrong type of ECT.
Because of the absence of valid and scientific studies by impartial doctors, and the seeming political unlikelihood that such studies will ever happen, survivors of ECT have had to take the lead in designing and implementing our own research. In the past several years there have been four large studies which focused on amnesia and memory disability. All of these went to a heterogeneous group of survivors, from people who'd had ECT in the past year to those who'd had it twenty years ago. One was done in the US by Juli Lawrence, an ECT survivor and member of the Center for Mental Health Services Advisory Board; three were done in England. The findings of all of these independent studies have been strikingly similar.
In my own study which I designed, I sent an questionnaire commonly used to assess brain injury, slightly modified to include the most common ECT symptoms, to our members, and every one of the 51 people who responded reported having at least some of the symptoms. Two-thirds had become unemployed due to ECT. 90% said they wanted and needed help with their cognitive and memory deficits, and had been unable to get it.
The United Kingdom Advocacy Network, a patients rights group in England, surveyed 308 survivors of ECT, one-third of whom had received forced shock. 60% of women and 46% of men found ECT damaging or not helpful. 73% reported permanent memory loss. 78% said they would never agree to ECT again.
Juli Lawrence's study of 41 survivors found that 70% had not been helped by ECT. 83% reported permanent memory loss, in some cases up to 20 years of amnesia. 64% reported permanent problems with memory functioning. 43% said ECT had caused permanent changes in cognitive abilities.
ECT Anonymous is the sister group to the Committee for Truth in Psychiatry in the UK. It is entirely made up of ECT survivors. They designed an extensive survey which as of 1999 has been completed by about 225 people. 82% reported permanent memory loss; 81% reported permanent memory disability; 50 to 80% reported permanent impairment in various cognitive abilities; 73% reported that ECT was not helpful in any longterm way. 76% were never able to return to their previous occupations.
MIND is a British charity which might be compared to our Mental Health Associations. In 2001, they published their survey of 418 ECT survivors. One-third had ECT against their will. 84% reported permanent adverse effects, including amnesia and cognitive deficits. 43% of the total found ECT unhelpful, damaging or severely damaging, and 65% said they would not have it again.
There is another adverse effect even more chilling than losing years of your life, and that is death. We don't have accurate national figures on deaths from ECT, because we don't collect any national statistics on ECT. Those that you may have heard are either an industry projection based on very old numbers (like the claimed "100,000 people get ECT a year) or a complete fabrication (like the death rate claimed by the APA). Only six states are required to report deaths from ECT, and not all of them have up-to-date figures. Texas is one state that has kept statistics in recent years, and they show a death rate of 1 in 200. In 1998, Illinois reported a death rate of 1 in 550. Yet patients are never told of these statistics.
A large retrospective study of 3,228 ECT patients in Monroe County, New York found that ECT recipients had an increased death rate from all causes. Another large study corroborated the fact that ECT survivors die sooner than mental patients who haven't had ECT. There is research to show that ECT survivors relapse more quickly than patients who were treated with drugs, and are much more likely to commit suicide. There is research that suggests that ECT survivors are more likely to develop Alzheimer's disease. There is no research on other longterm adverse effects of ECT, such as its longterm effects on the heart. If someone such as myself develops a heart condition at an early age, a condition for which there is no risk factor or family history, is this a result of ECT? No one's even looking into this.
To summarize what we know about adverse effects: 100% of persons who have ECT experience permanent memory loss, and a majority experience significant, extensive loss. Memory lost to ECT doesn't "return". NIMH looked at what the industry says and estimated that the average period permanently lost to ECT is eight months. That's an underestimate, as you'd expect. It is frequent, not rare, for persons to lose many years of their life to ECT, and for this loss to be permanently disabling. ECT commonly causes many of the other permanent effects typical of brain injuries, including loss of intelligence, permanently impaired memory functioning, and other cognitive problems which is sum amount to preventable disability.
What about efficacy? Are there benefits to ECT that can justify these risks?
Let's look at what the industry itself says. You may have heard a claim that ECT prevents suicide or saves lives. It doesn't. There is not one study to prove this. In fact, the industry-designed research shows the opposite: ECT has no effect on suicide, at least as far as preventing it. There are many, many studies that document suicide after ECT, often when researchers attempt to find their patients a month or three afterwards and can't find a certain percentage of their patients because they've killed themselves. Ernest Hemingway is just the most famous example of a suicide caused by ECT.
In 1985, NIMH looked at the published research---again, this is research largely done by the industry itself---and concluded that there was no evidence that ECT has any beneficial effects that last longer than four weeks. In 1992, two British psychiatrists presented a paper at an international conference, evaluating all the studies that had been done up to then---there have been none since---which compared real ECT to what's called sham ECT (anesthesia alone without electricity). They concluded that there is no evidence that real ECT is superior to fake ECT. Remember, in both cases all that was being evaluated was ECT's efficacy in depression, the condition for which is it supposedly most effective; ECT is commonly used for other conditions for which it is considered less effective, as in the case of Paul Henry Thomas.
ECT's lack of efficacy is a big public relations problem for the industry. In 2001, the industry's leading spokeman Harold Sackeim published a paper looking at what happens to patients who've had ECT. This study was based on research done from 1992 to 1998, and I remind you that this research was done in violation of federal law. I have also examined the grant file for this study, and I can tell you that the actual results reported to NIMH do not match the results revealed to the public in the published study. I can't tell you why, or what happened to the patients who were disappeared, except to ask you to look into it.
The point here is not that this study is good science, or that you should believe what it says, but that it was the best that the most prominent and best-funded spokesman of the ECT industry, using millions of our tax dollars, could come up with.
Of the roughly 290 people who were shocked for this study, half did not respond to ECT at all. That's a 50 percent response rate for the very definition of state-of-the-art, 21st century ECT. But in fact Dr. Sackeim cheated a bit, because he uses the special shock machines that he designs to put out twice as much electricity as patients normally get. This, as Sackeim would tell you, boosted the response rate higher than it would have been in clinical use----but it was still only 50%. (Correspondingly, when a study focuses on cognitive effects and not efficacy, researchers are able to turn down the electricity to less than is given in normal practice.)
Of the roughly 150 people who responded to ECT, only about 25 (we don't know the exact number because Sackeim says different things in different places) were free of depression six months after shock. An equal number, about 21, had become so depressed again that they had more shock within six months. That's a total of only about 10% of the total who had any benefit from shock that lasted as long as six months.
The study notes that most patients who relapsed did so very quickly. This is consistent with earlier studies. NIMH reviewed these studies and concluded that there is no scientific evidence that any benefit of ECT lasts longer than four weeks.
It has been noted by numerous scientists that this extremely brief period of well being is entirely consistent what is seen in other types of brain injuries, and with the theory that ECT "works" by causing an acute organic brain syndrome.
In contrast to benefits, the adverse effects of ECT are permanent. At any length of time at which survivors have been followed up post-ECT, the vast majority report a stable retrograde amnesia for months or years. When survivors have been tested with instruments sensitive to brain injury at any length of time post-ECT, they have exhibited stable and permanent deficits in intelligence, memory ability, abstract thinking and other cognitive functions, and the pattern of impairment is consistent among survivors no matter when or where they had ECT. All of the adverse effect reports collected by the FDA are of permanent, enduring deficits. The effects of electricity on the human brain have not been mitigated by any claimed improvements or refinements by the industry. There is a great deal of variance among individual ECT patients, because the amount of electricity received varies greatly and cannot be controlled by even the most modern devices, due to human physiology and the nature of electricity. There is no way to predict who will be most devastated by ECT.
ECT's morbidity rate is 100%. It commonly results in permanent disability, and lifetime Social Security payments, in adults who previously were able to work. Its mortality rate, based on very spotty statistics, may be as high as 1 in 200. ECT has not been shown to be more effective than no treatment at all, and even the most biased estimate of its longterm efficacy rate is only 10 to 40%.
You would be right if you guessed that the FDA has placed the ECT device in its Class III, High Risk category. FDA warns that the benefits of ECT do not outweigh its risks and that its risks include brain damage and memory loss.
If ECT were a drug just coming on to the market, it would not be allowed to be used.
If safety trials of a drug showed that the drug caused permanent amnesia, disability, and brain damage in even a small fraction of those who have experienced these effects due to ECT, that drug would be pulled off the market.
Would it surprise you at this point to learn that there have never been any safety trials of the ECT device? There have not. None of the manufacturers of the devices have ever conducted a single safety test. (When manufacturers, in their ads, say their devices are safe, they mean safe for the treating psychiatrists and nurses!) Even in 1997, when the FDA belatedly called for them to submit safety information, they did not submit one shred of evidence, because there is none. They knew there would be no consequences for not submitting the required information, and there have been none. If the ECT device didn't have the powerful lobby of the American Psychiatric Association behind it, it would be pulled off the market.
You may rightly ask why ECT continues to be used given its terrible track record. There are many reasons. One is the historical quirk that ECT was invented in fascist Italy, at a time and place where there were no protections for patients and no regulation of industry, that it continued to be used free of the restrictions and protections we take for granted in this country, and that today it is still largely immune from such restrictions and protections. We can't even get the most basic information about the use of ECT in New York State today, such as how much it's done!
In 1976 the APA formed its Task Force on ECT, and since then ECT has been kept alive largely by vigorous sustained effort on the part of a dozen men who design the machines, conduct the research, consult for the companies, and otherwise owe their highly paid lifestyles to ECT. New York State is home to two men in particular who have staked everything on ECT and have everything to lose if it is discredited. It's the shame of our state and part of the reason all attempts at patient protection here have failed so far. Both men are or were state employees. No wonder OMH is so invested in the forced shock of Paul Thomas, Adam Szyszko, and so many others.
Fink and Sackeim and a few others around the country are so busy promoting ECT, lying to the media, conducting big ticket how-to-do-shock seminars, etc., because if they let up on their public relations campaign for a minute ECT would collapse under the weight of all the scientific evidence against it.
Did I mention how enormously profitable it is? Medical journals recommend setting up "ECT suites" to bolster incomes threatened by managed care. Insurance companies pay for ECT without asking questions, and that's not an accident; the proponents of ECT, such as Dr. Fink, are consultants to the insurance companies. Psychiatrists who do ECT make an average of twice the income of those who don't use it, and they can achieve this increase in income by working only the few hours a week it takes to give a bunch of treatments. It's easy to set up an ECT practice; all you have to do is pay about a thousand dollars to Drs. Fink, Sackeim, Weiner, etc.; go to the seminar for a few hours, pass the test and you're considered qualified to do ECT. This practice bears further scrutiny by the Assembly.
As a society, we allow things to be done to mental patients that would be unconscionable if done to persons without psychiatric labels. Hatred and fear of mental patients is so ingrained among the general population, and so unquestioned, it's never recognized for what it is, except by those of us who are on the receiving end of it every day. Getting a psychiatric label is like having a curse placed on you: from this day on, as long as you live, you will not be believed. You may dismiss my testimony and that of my peers, if you wish, as the ravings of an irrational crazy person, without compunction, because it's socially acceptable for you to do so. You may place less value on the brain and life of Paul Henri Thomas than you would on your own, and that again is socially acceptable. You may even do these things without conscious awareness that you are doing them. This is how shock and forced shock came to be, and how they continue.
Along these lines, I warn you not to derail these hearings into a general discussion of mental patient competency---as happened to some extent in 1977. Too often, the discussion on informed consent to shock ends when someone assumes that the real issue is that mental patients lack capacity to consent to anything. First of all, that's not true in the vast majority of cases. Second, it implies that the problem with shock resides in the patient, and not the industry. In 2001, the sharpest, most alert, most intelligent and competent patient cannot give informed consent to ECT, because there is nowhere in New York State or in the country where that patient will be informed of the true risks and benefits of shock. The patient is deceived by the assurances provided by the shock industry that shock is effective, that memory loss is trivial and rare, that memory comes back...the lies propagated by the APA's small Task Force of career ECT promoters. Until the day when the most competent patient can give informed consent to shock, no one can.
There is one more reason why ECT continues to exist. Psychiatrists need it. There are always going to be people whom they cannot help, and the more the field comes to rely exclusively on biological theories of mental illness and biological treatments, the more true this will be. There must be something psychiatry can hold out to those it has failed (and it is they who have failed, despite their practice of referring to their patients as "treatment failures")---something drastic and dramatic, something absolutely certain to have a dramatic effect in the short term, some last resort that can get the patient out of the hospital in the time allotted by the insurance companies and make the psychiatrist look like a hero. If a patient's brain is damaged in the process, that is a small price to pay (for the psychiatrist). Psychiatry offers brain damage as treatment because it has nothing else to offer. It is bankrupt. I am sure that if psychiatry could come up with something else besides ECT that fit the need for the last-resort treatment, it would get rid of shock. It's been trying for decades and hasn't come up with anything. Dr. Sackeim and others who have tried to develop (and profit from) drugs to eliminate the adverse effects of ECT have been unsuccessful. He's currently experimenting with giant magnets. But psychiatry's not going to admit ECT is brain damage until it has something else to offer. It puts saving face ahead of saving patients' brains.
Contact information:
Linda Andre
Committee for Truth in Psychiatry
P.O. Box 1214
New York, NY 10003
212 665-6587
ctip@erols.com
next: The Identification and Management of Patients with a High Risk for Cardiac Arrhythmias During Modified ECT
~ all Shocked! ECT articles
~ depression library articles
~ all articles on depression
APA Reference
Staff, H.
(2001, May 18). Testimony of Linda Andre, Director of Committee for Truth in Psychiatry, HealthyPlace. Retrieved
on 2024, December 21 from https://www.healthyplace.com/depression/articles/testimony-of-linda-andre-director-of-committee-for-truth-in-psychiatry